
Symptoms and different forms
The symptoms can manifest themselves in many different degrees and variants, and a distinction has traditionally been drawn between two main types of leprosy: the lepromatous and the tuberculoid forms. Without treatment, the disease will gradually worsen and may result in permanent injury and disability.
Modes of infection
Transmission mainly occurs through droplet infection, but the risk of transmission is low and usually requires close and prolonged contact with the infected person. Even then, only a small proportion of those infected become ill. For the disease to develop, several conditions must be present in addition to the bacterium, and nutrition and genetics are decisive additional factors.
A disease with many names
Leprosy or Hansen’s disease? The disease and the people affected by it have been known by different names throughout the ages, both in the medical community and among the general population. It is important to be aware of the terms we use, as older terms may be considered offensive today.
One disease, many myths
Leprosy is one of the oldest known diseases and has often been associated with religious and social stigmas. People all over the world have experienced the disease having major social consequences, but far from all were ostracized or isolated. Many of those who experienced leprosy received support and help from their families, communities and others.

Miasma, climate or fatty fish?
The miasma theory remained prevalent until well into the 19th century. Many believed Miasma to be a substance that manifested in unhealthy places in nature and that could induce disease, while others pointed to climatic conditions.
Heredity?
Danielssen observed that a large proportion of the residents at St. Jørgen’s Hospital had family members or other relatives with the same disease, although he did not observe hospital staff or others in contact with patients being infected. Danielssen therefore concluded that leprosy was a hereditary blood disease.
Contagion?
One of the first to advocate that leprosy was infectious was Ove Guldberg Høegh, the father of the National Leprosy Registry of Norway. The registry enabled Armauer Hansen to demonstrate that isolation through hospitalisation reduced the number of new leprosy cases, indicating that the disease was infectious.
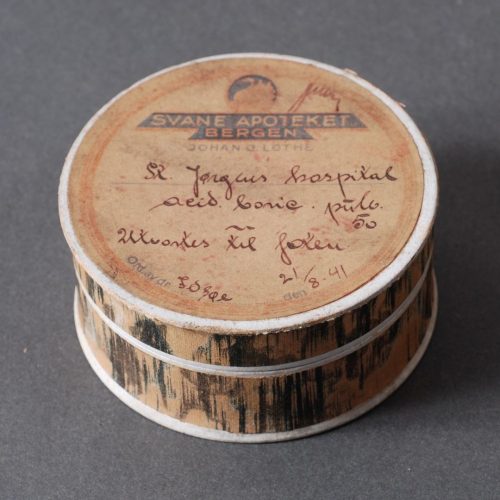
Quicksilver and charlatans
A number of the city physicians attempted to cure some of the residents at St. Jørgen’s Hospital as early as the first decades of the 18th century. They initially placed most emphasis on diet, but bathing and mercury treatment were later trialled. A number of well-known charlatans – with no medical education – also offered various treatments.
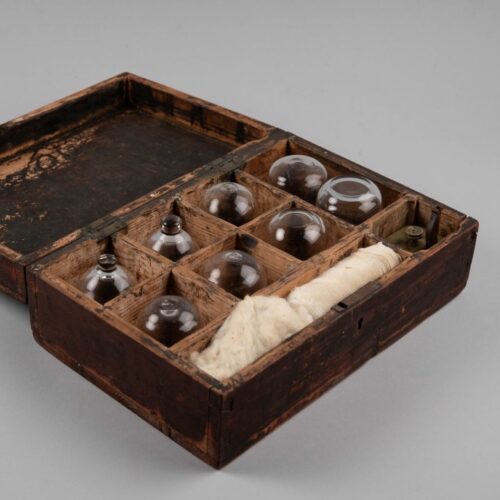
Cupping and bloodletting
Bloodletting was a common treatment method in times past. It involved draining varying amounts of blood from the patient. The procedure could be performed using leeches, by making incisions in the skin that would be left to bleed, or by cupping. Cupping involved small incisions being made in the skin before a hollow object was placed over the wounds to draw blood.

‘Reluctance’ to curative trials
The annual reports of the doctors associated with St. Jørgen’s Hospital describe the residents not following the doctors’ suggestions for possible treatments, nor advice about diet and hygiene. They describe in particular how patients had little inclination to take medicine over a prolonged period, despite the doctors’ attempts to persuade them.
Resistance to autopsies
If many of the residents at St. Jørgen’s Hospital were sceptical about trying new treatments, they had even more reservations about autopsies – which at that time were also referred to as ‘corpse examinations’ or ‘sections’. When Danielssen wanted to start carrying out autopsies in the 1840s, he was met with shock, fear, and outrage.
The book ‘On Leprosy’ from 1847
The written work was the first modern scientific description of leprosy and formed the basis for leprosy research for a long time to come. Leprosy was defined for the first time as a specific disease and clearly distinguished from other skin conditions. The book was published in both Norwegian and French, earning international recognition for its authors, Danielssen and Boeck.
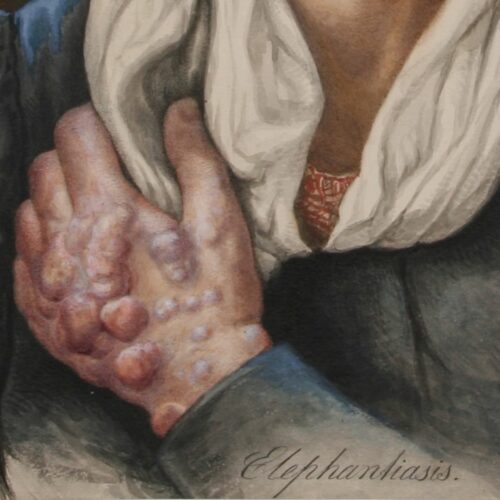
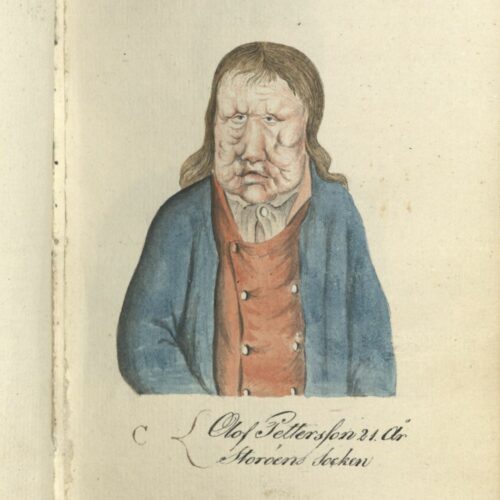
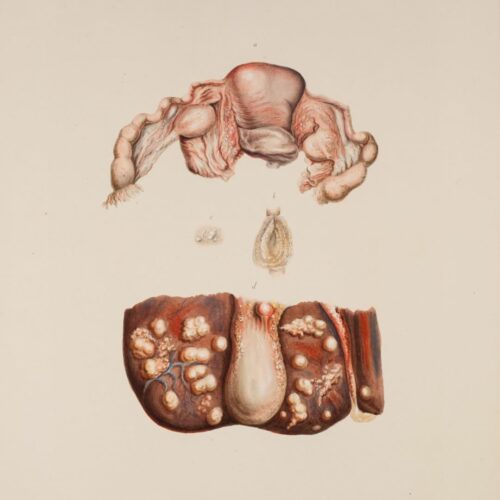
‘Atlas Colorié de Spedalskhed’
The atlas accompanied the book ‘On Leprosy’ and contains 24 colour plates depicting the external characteristics of the disease as observed in the residents at St. Jørgen’s Hospital in the 1840s. The watercolours were painted by the artist and lithographer Johan Ludvig Losting and engraved at Prahl’s lithographic workshop in Bergen.
The journal ‘Medicinsk Revue’.
This Norwegian medical journal was established by four doctors in Bergen in 1884, including Eduard Bøckmann and Gerhard Armauer Hansen. The journal contained some original works by Norwegian scientists but was largely based on the reproduction of summaries of international research. The scientific library at Lungegård Hospital played an important role.
The leprosy registry
Collecting and analysing information about everyone who had leprosy in Norway was time-consuming, both for district medical officers and the Chief Medical Officer for Leprosy, but it provided new and valuable knowledge for health authorities and medical experts. The Leprosy Registry is considered the first ever national patient registry. It served as a model for other registries and illustrates the important role that health registries play in epidemiological research and public health.
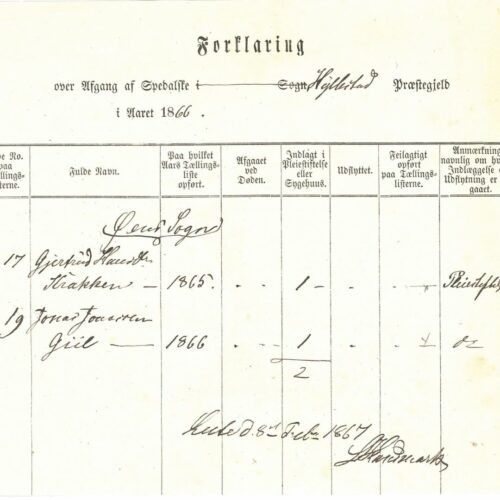
System of registration
District Medical Officers, aided by local pastors and health commissions, were to create detailed overviews of everyone afflicted with leprosy. There were several different forms for registering information, containing a number of columns that had to be filled in. Reports from across the country were then added to and organised in central registries, which were used by the Chief Medical Officer to produce and publish statistical material.
‘The Chief Medical Officer for Leprosy’
The Chief Medical Officer was to work on combating leprosy and propose measures that could help eradicate the disease. Central duties included the operation of the state care institutions and the administration and analyses of the leprosy registry data. A total of five doctors held the office between 1854 and 1957, ensuring continuity of the state’s efforts to combat the disease.
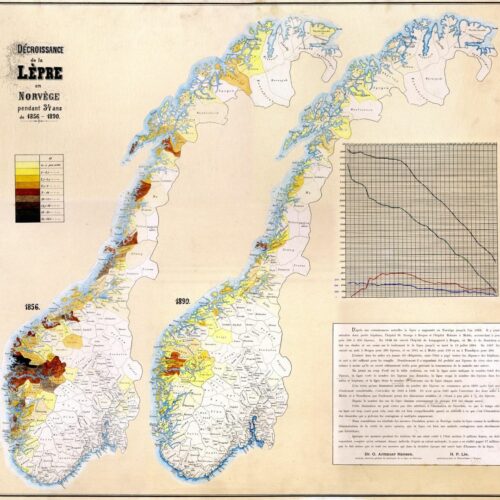
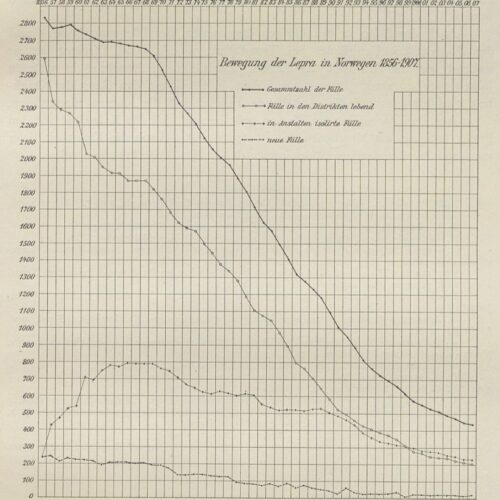
The registry’s significance
The registry became an important tool in the health authorities’ efforts to limit the spread of the disease, making it possible to continuously monitor the prevalence in different geographical areas and to observe the effect of the measures implemented. Analyses of the registry’s data were also pivotal to Hansen’s argument that the disease was infectious and that isolation was a recommended measure.

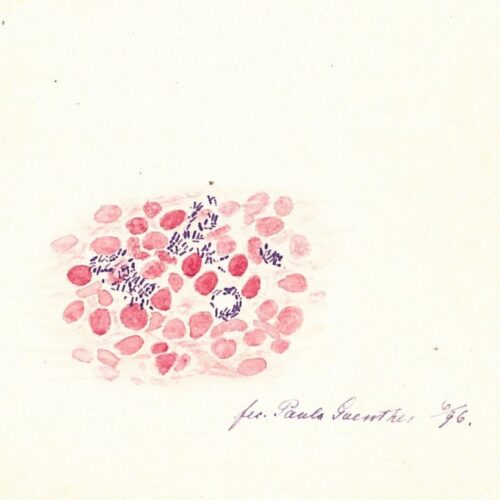
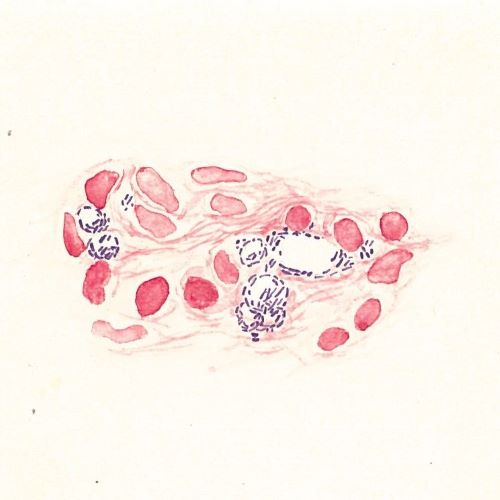
Identifying an infectious agent
Even before Hansen was employed as a physician at several leprosy hospitals in 1868, he was already convinced that the disease was caused by an infectious agent. If that was the case, the agent should be detectable in diseased organisms. The question remained, however, of where precisely in the patient he should look and what type of infectious agent he should be trying to find.
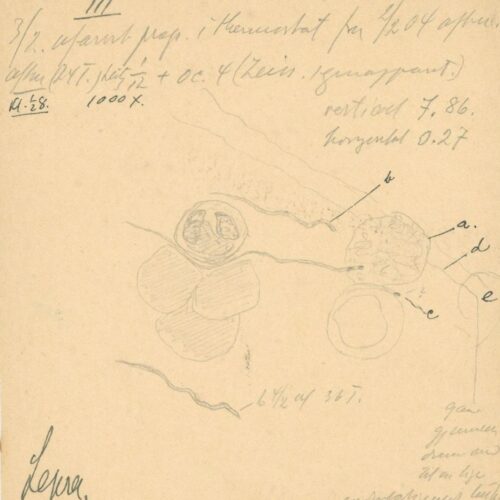
Making the invisible visible
The microscope technology of the day made it possible to search for an infectious agent. Microscopes had significantly improved and researchers had gained a clearer understanding of microorganisms. This laid the groundwork for developing scientific principles for proving the link between microorganisms and disease.
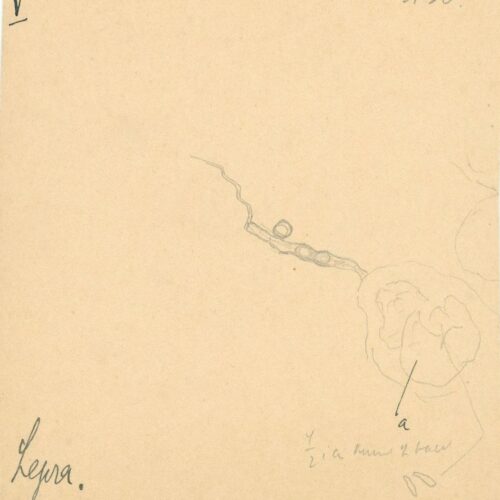
The search for evidence
In order to prove that bacteria was the cause of leprosy, it was not enough to merely observe them under a microscope. It was also necessary to observe them causing the disease. In November 1879, Hansen summoned the patient Kari Nilsdatter Spidsøen into his office at Pleiestiftelsen Hospital. Against her will, he inserted leprosy-infected material into the conjunctiva of her eye.
Trial, verdict and ethics
Armauer Hansen’s experiment on Kari Nilsdatter had legal consequences. He was charged with bodily harm, but he was only convicted of abuse of office. He lost his position as physician at Pleiestiftelsen Hospital but remained in his post as Chief Medical Officer for Leprosy. Although the verdict has since been considered groundbreaking for patients’ rights, it was not widely discussed publicly in its day.
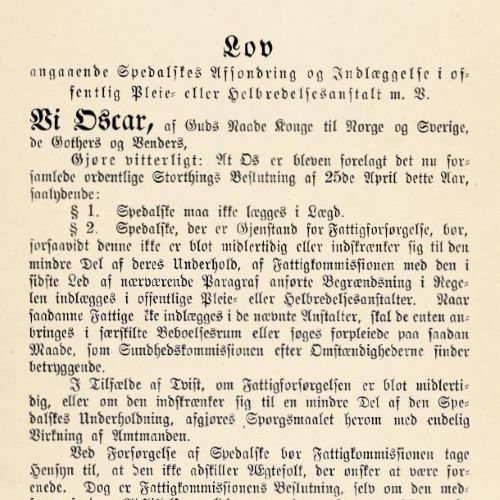
Leprosy legislation
A new leprosy act from 1885 was the first Norwegian act to permit the use of force in relation to the chronically ill. This provoked debate, even though force could only be used in instances where it was deemed necessary to prevent transmission. People affected by leprosy could continue to live at home on the condition that they lived ‘in satisfactory isolation from their family and surroundings’.
Humane legislation?
There was lively debate about the new legislation. Many believed the act was too strict and protested against it ‘in the name of humanity’. Its most critical opponents alleged the act likened those affected by leprosy to convicts. Hansen, who had formulated the principles behind the act, made the case that one could not only consider those who had leprosy, but that they also had a duty to protect their fellow citizens.
Coercion or education?
The coercion clause was not used to any great extent, but the act had a potential educative effect on those who were living at home. They could remain at home on the condition that they ensured a safe distance from others. If they exercised a greater degree of caution in their contact with others to avoid hospitalisation, this would help reduce the risk of transmission.
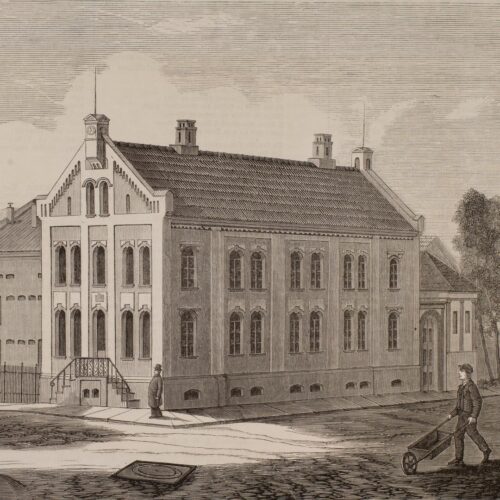
Isolation – at home or in hospital
Although Norway was seen as a role model when it came to using isolation as a means of combating the disease, at no point were all those registered with the disease admitted to hospitals or care institutions. It wasn’t until some point between 1890 and 1900 that more people with leprosy were staying in hospitals than living at home in their local communities.
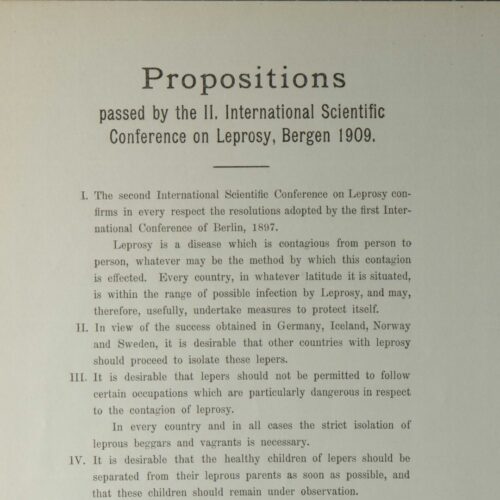
The leprosy act – a role model?
The Norwegian legislation garnered world-wide interest and to some extent inspired much stricter legislation in other countries. Debates and resolutions at the International Leprosy Conferences in Berlin in 1897 and in Bergen in 1909 led to an agreement to recommend compulsory registration and isolation of those affected by leprosy. But was this not based on a somewhat simplistic view?

The Leprosy Conference in Bergen
The second International Leprosy Conference was held in Bergen in August 1909. For four days, almost 180 participants from 30 countries and four continents came together, including numerous prominent medical figures of the time. The conference’s proceedings were printed in three volumes. They show that Armauer Hansen’s argument that leprosy was an infectious disease had gained traction all over the world.